Abstract
A case of acute necrotising pancreatitis, was admitted in our tertiary care centre with complaints of abdominal pain in the epigastric region for 2 days. Pain was associated with vomiting, sore throat and fever on and off. On examination, the patient was tachycardic, and had B/L parotid enlargement with erythema. Systemic examination was insignificant except for mild epigastric tenderness and distension. USG and CECT- abdomen confirmed the necrotising nature of the pancreatitis. The biochemical and serological work-up eventually revealed the final diagnosis of the cause of pancreatitis in the patient. The case is being published in view of the rarity, and the difficulty in diagnosing the condition. Keywords: Acute necrotizing, Abdominal pain
INTRODUCTION
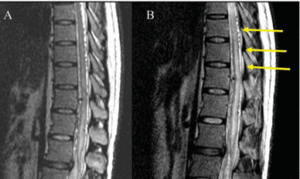
A 15 year old male, referred as a case of acute necrotising pancreatitis, was admitted in our tertiary care centre with complaints of abdominal pain in the epigastric region for 2 days. Pain was associated with vomiting, sore throat and fever on and off. Patient did not have any significant past medical/surgical history and was non-alcoholic. Patient was immunised only for BCG and OPV. On examination, the patient was tachycardic, and had B/L parotid enlargement with erythema. Systemic examination was insignificant except for mild epigastric tenderness and distension. USG and CECT- abdomen confirmed the necrotising nature of the pancreatitis associated with pleural effusion (BISAP score – 2/5). On biochemical examination, Lipid profile, Sr. Calcium, PTH were found to be normal. The regular fever panel (for Dengue, Malaria, Typhoid, Filaria and Leptospira), Blood and Urine C/S were negative. Mumps IgM and IgG ELISA was done, in view of the clinical findings and it turned out to be positive. The patient was treated conservatively, with serial monitoring of Sr. Amylase and Lipase, and discharged upon radiological evidence of disease remission. After 1967 (Post-vaccination era), USA’s CDC has reported only 1 notified case of mumps pancreatitis, as per available literature1. Mumps pancreatitis, which may present as abdominal pain, occurs in ~4% of infections but is difficult to diagnose because an elevated serum amylase level can be associated with either parotitis or pancreatitis2. In 1817, mumps virus was implicated for the first time as a cause of acute pancreatitis. Diagnosis is based mainly on detecting anti-viral antibodies, the clinical picture, imaging of the pancreas and finally on the exclusion of other causes of pancreatitis3. The case is being published in view of the rarity, and the difficulty in diagnosing the condition.
REFERENCES:
1. Taii A1, Sakagami J, Mitsufuji S, Kataoka K, Acute pancreatitis from mumps re
infection in adulthood. A case report.; JOP (Journal of Pancreas). 2008 May
8;9(3):322-6;
2. Stephen L. Hauser, Tinsley R. Harrison, Eugene Braunwald, Harrison’s Principles of
Medicine, 19/e, 231e-3.
3. M. Economou, M. Zissis, Infectious causes of Acute Pancreatitis, ANNALS OF
GASTROENTEROLOGY 2000, 13(2); 98-101.
4. Feldstein JD, Johnson FR, Kallick CA, Doolas A. Acute hemorrhagic pancreatitis and
pseudocyst due to mumps. Ann Surg 1974;180: 85–8.
5. G Rajesh, Asha S Nair, V A Narayanan, V Balakrishnan Acute pancreatitis in viral
infections, with possible progression to chronic pancreatitis Indian Journal of
Gastroenterology 2008 Vol 27 Number 4 162-4.
1. Taii A1, Sakagami J, Mitsufuji S, Kataoka K, Acute pancreatitis from mumps re
infection in adulthood. A case report.; JOP (Journal of Pancreas). 2008 May
8;9(3):322-6;
2. Stephen L. Hauser, Tinsley R. Harrison, Eugene Braunwald, Harrison’s Principles of
Medicine, 19/e, 231e-3.
3. M. Economou, M. Zissis, Infectious causes of Acute Pancreatitis, ANNALS OF
GASTROENTEROLOGY 2000, 13(2); 98-101.
4. Feldstein JD, Johnson FR, Kallick CA, Doolas A. Acute hemorrhagic pancreatitis and
pseudocyst due to mumps. Ann Surg 1974;180: 85–8.
5. G Rajesh, Asha S Nair, V A Narayanan, V Balakrishnan Acute pancreatitis in viral
infections, with possible progression to chronic pancreatitis Indian Journal of
Gastroenterology 2008 Vol 27 Number 4 162-4.